Targeted muscle reinnervation pain control surgery
Get in touch
Despite the large variety of surgical treatments which have been proposed to address the debilitating effects of neuroma pain after an amputation, the only surgical treatment which has been shown to result in a consistent and reproducible improvement is Targeted Muscle Reinnervation (TMR) surgery.
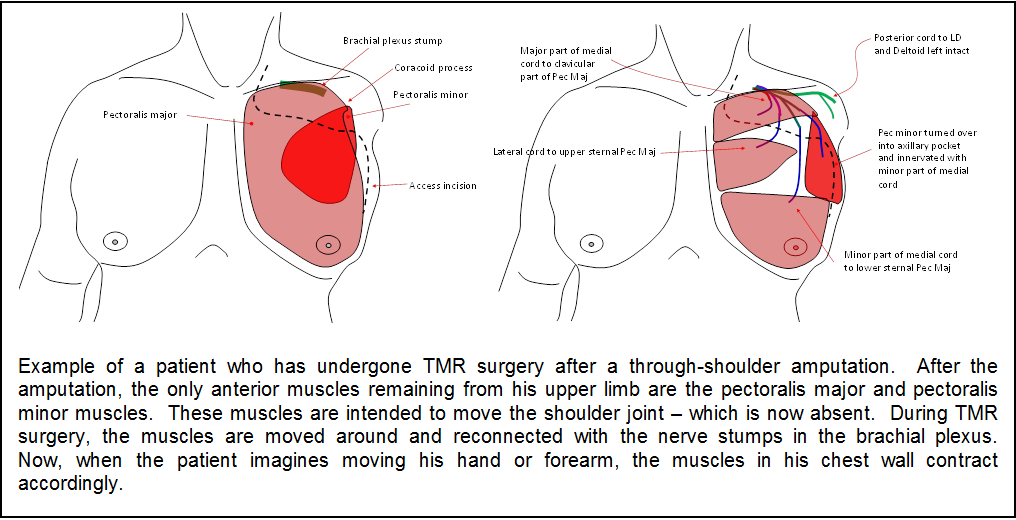
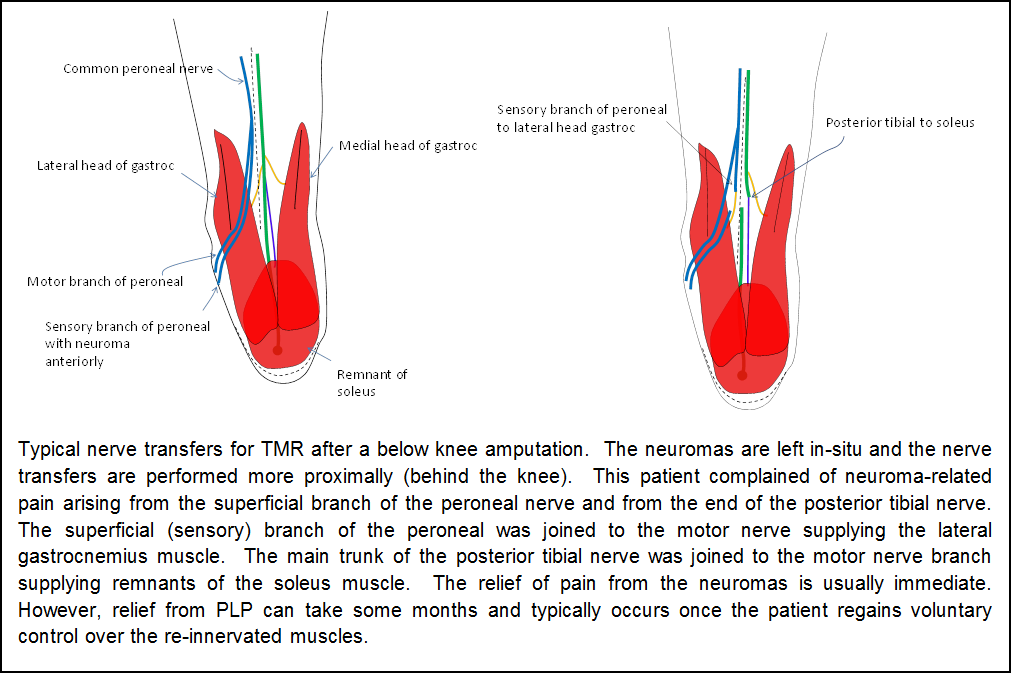
The TMR procedure involves transferring the large peripheral nerve stumps in the amputation stump and connecting them to the motor nerves of carefully selected target muscles within or close to the residual limb (stump). The target muscles that we select are usually muscles in the residual limb whose function is now redundant because of the amputation (i.e. they were intended to move parts of the limb which no longer exist – for example biceps after a trans humeral amputation).
Despite the large variety of surgical treatments which have been proposed to address the debilitating effects of neuroma pain after an amputation, the only surgical treatment which has been shown to result in a consistent and reproducible improvement is Targeted Muscle Reinnervation (TMR) surgery.
The TMR procedure involves transferring the large peripheral nerve stumps in the amputation stump and connecting them to the motor nerves of carefully selected target muscles within or close to the residual limb (stump). The target muscles that we select are usually muscles in the residual limb whose function is now redundant because of the amputation (i.e. they were intended to move parts of the limb which no longer exist – for example biceps after a trans humeral amputation).
Aftercare/pain Control
Patients undergoing TMR surgery alone (i.e. not in combination with Osseointegration) will generally go home on the same day as surgery. The only exception is for patients with a very high transhumeral or through shoulder amputation where it is likely that they will need to have exploration of their brachial plexus. Such patients will need to be admitted overnight for pain control.
Patients undergoing TMR surgery alone will need to take all their normal pain medications before surgery and should expect a significant increase in their phantom limb pain which may be maximal at 3 – 6 months after treatment. We advise our patients that they will need to increase their intake of pain medications (such as pregabalin) in line with their symptoms and may wish to consider doing so 1 -2 weeks before the surgery is performed. The actual pain of surgery is usually minimal and easily controlled with simple analgesics or mild opiates – taken for a few days.
After TMR surgery, your incision will be closed (typically) with absorbable sutures which do not need to be removed. You may wash and shower with running water immediately after surgery but should avoid any heavy use of the limb for 2-3 weeks. Importantly, you must not use your prosthesis until the wound has healed (3 weeks) and any associated soft-tissue swelling has resolved.
Detectable reinnervation of the muscles will occur as early as 4 weeks after surgery but will reach a maximum at 12 – 18 months. During that time, patients who are having TMR surgery for improvement of bionic limb control must undergo close rehabilitation with a rehabilitation unit that is experienced in the use of computerised feedback techniques. This will allow the amputee to learn to use the reinnvervated muscles to the best of their ability and helps to reinforce and strengthen the reinnvervation pathways.
You do not need any specific rehabilitation exercises if you are undergoing TMR surgery to deal with neuroma pain. However, it has been our experience that patients who learn to use their reinnervated muscles quickly also observe more rapid resolution of their phantom limb pain.